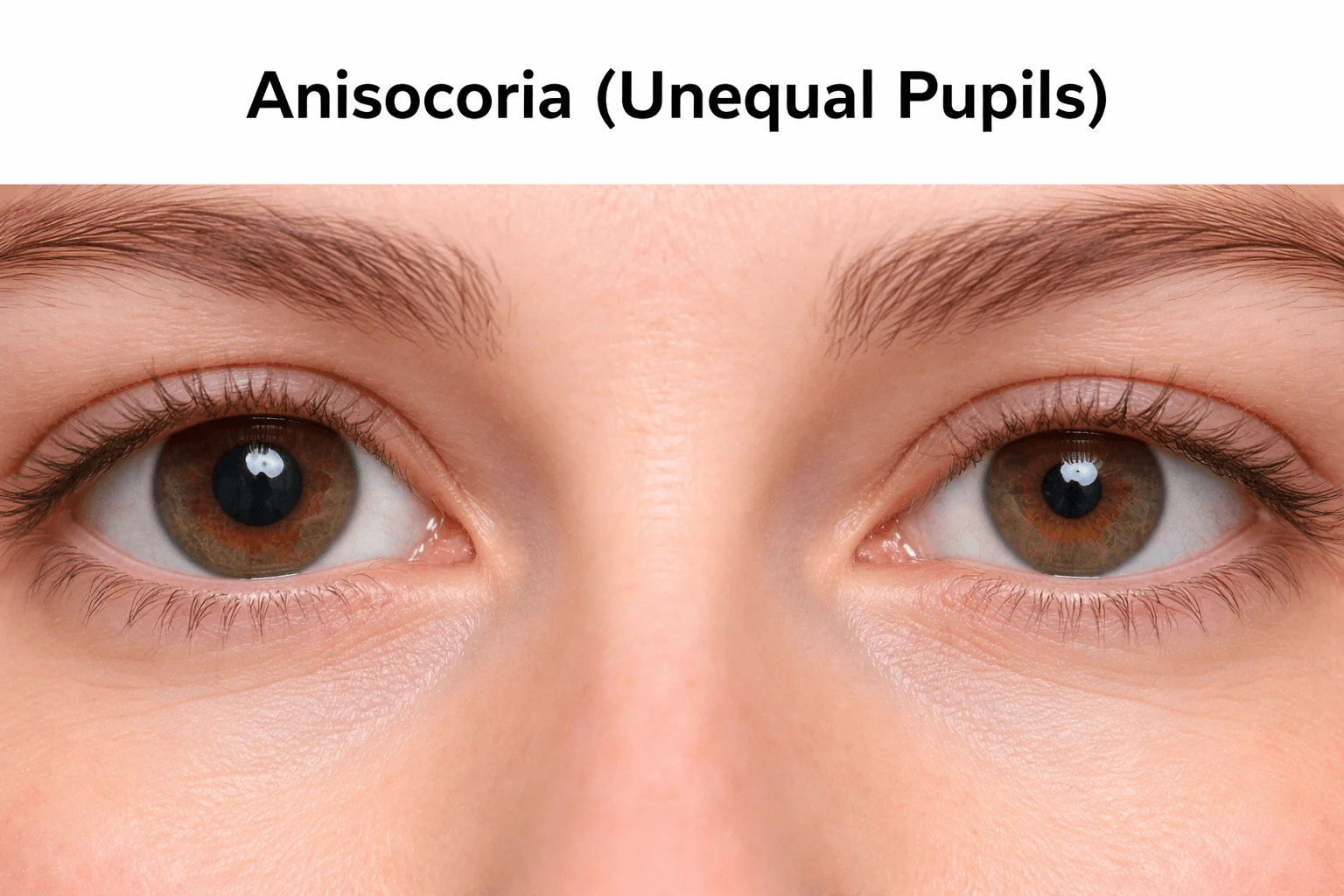
Anisocoria (Unequal Pupils)
A difference in pupil size between the two eyes. Most often harmless, but the right pattern can point to Horner syndrome, an Adie tonic pupil, or a third nerve palsy - one of which is a medical emergency.
Anisocoria simply means the two pupils are different sizes. It is one of the most common findings in clinic, and most of the time it is harmless - a normal variant present in a meaningful fraction of healthy people. The job of the evaluation is not to panic at every size difference but to sort the harmless cases from the few that signal a problem in the nerves that control the pupil. Done methodically, that sorting is fast and reliable, and it hinges on a handful of questions: which pupil is the abnormal one, does the difference change with lighting, and are there warning signs that demand emergency care.
Key takeaways
- A pupil-size difference is often physiologic - benign, longstanding, and present in roughly a fifth of people
- The first decision is which pupil is abnormal, answered by comparing the difference in bright light versus darkness
- The three patterns to triage are Horner syndrome, an Adie tonic pupil, and a third nerve palsy - very different in cause and urgency
- A newly dilated pupil with a droopy lid and double vision can mean an aneurysm pressing on the third nerve and is an emergency
- Old photos and a medication list are genuinely useful - many cases are solved by showing the difference is old or drop-related
Questions about your diagnosis? Contact our office
For a broader walk-through of pupil problems and what to expect during evaluation, see our guide: Understanding Pupil Abnormalities - When Unequal Pupils Need Attention.
Call 911 or get to an emergency department immediately if a newly enlarged pupil appears together with a drooping eyelid and double vision, or with a sudden, severe "worst headache of my life." This combination can mean an aneurysm compressing the third cranial nerve, which can rupture and is life-threatening. New unequal pupils after head trauma, or with weakness, slurred speech, or confusion, also need emergency care.
Step One: Which Pupil Is the Abnormal One?
When the pupils are unequal, one of them is behaving normally and the other is not - and identifying which is which immediately narrows the diagnosis. The trick is to compare the size difference under two lighting conditions, because the pupil's two opposing muscles fail in opposite settings.
- If the difference is greater in bright light, the larger pupil is the abnormal one. It is failing to constrict the way it should when light hits it. This points toward a third nerve palsy, an Adie tonic pupil, or pharmacologic dilation from a drop or substance.
- If the difference is greater in the dark, the smaller pupil is the abnormal one. It is failing to dilate as it should in dim light. This points toward Horner syndrome, pharmacologic constriction, or scarring from old inflammation.
- If the difference is the same in light and dark and both pupils react briskly, the finding is usually physiologic anisocoria - benign and not a sign of disease.
The Three Patterns to Triage
Horner Syndrome - the Smaller, Sluggishly Dilating Pupil
Horner syndrome comes from interruption of the sympathetic pathway that dilates the pupil and lifts the lid. The affected pupil is smaller, the difference is more obvious in the dark (because it lags in dilating), and it is typically accompanied by a mild droop of the upper lid on the same side and sometimes reduced sweating of that side of the face. Horner syndrome is itself only a sign; the underlying cause ranges from benign to serious, and a painful, sudden Horner syndrome with neck pain can indicate a carotid artery dissection, which needs prompt evaluation. The localization of the lesion - and therefore the workup - is part of what the neuro-ophthalmic exam sorts out.
Adie Tonic Pupil - the Larger, Slow Pupil in a Well Patient
An Adie (tonic) pupil results from damage to the parasympathetic supply to the iris, usually in an otherwise healthy young or middle-aged adult, often a woman. The affected pupil is larger, reacts poorly or not at all to light, and constricts slowly and then re-dilates slowly - the "tonic" behavior. A classic clue is light-near dissociation: the pupil responds better to a near focusing effort than to light. Adie pupil is generally benign, and when it occurs with diminished deep tendon reflexes it is called Adie syndrome. The crucial point is that it is not the dangerous cause of a dilated pupil.
Third Nerve Palsy - the Pattern That Can Be an Emergency
The third cranial nerve carries the fibers that constrict the pupil and also moves most of the eye and lifts the lid. When it is involved, the pupil can be large and poorly reactive, and - critically - this is often accompanied by a drooping eyelid and double vision from the eye sitting "down and out." A third nerve palsy that involves the pupil raises concern for a compressive lesion, classically an aneurysm of the posterior communicating artery, because the pupil-constricting fibers travel on the outer surface of the nerve where compression reaches them first. By contrast, the microvascular third nerve palsies seen with diabetes or high blood pressure more often spare the pupil. This "pupil rule" is helpful but not absolute - partial palsies and early cases can be ambiguous - which is why an acute third nerve palsy, especially with any pupil involvement, is treated as urgent and evaluated with prompt imaging of the brain and its blood vessels.
Pharmacologic Testing in Clinic
When the cause is not obvious from the exam, eye drops can confirm a diagnosis by exploiting how each pathway responds:
- Apraclonidine is used to confirm Horner syndrome. In Horner syndrome the affected pupil shows denervation supersensitivity and dilates with apraclonidine, often reversing the anisocoria - the smaller pupil becomes the larger one.
- Low-concentration (dilute) pilocarpine, around 0.1%, confirms an Adie tonic pupil: the supersensitive tonic pupil constricts to this weak solution, while a normal pupil does not.
- Standard 1% pilocarpine helps separate a pharmacologically dilated pupil from a third nerve palsy: a pupil dilated by an anticholinergic drop will not constrict to 1% pilocarpine, whereas a third nerve palsy pupil will. This is one reason it helps to know about any recent drop, patch, or plant exposure.
These tests are done by your eye doctor and interpreted alongside the rest of the exam; the timing between drops matters, so they are not something to attempt at home.
Other Causes Worth Knowing
- Pharmacologic effects are common culprits - scopolamine motion-sickness patches, nebulized ipratropium reaching the eye, glaucoma drops, and certain plant saps can all change pupil size, sometimes in only one eye.
- Eye inflammation (uveitis) and prior surgery or trauma can leave a pupil irregular and poorly reactive from scarring (synechiae) or iris damage.
- Argyll Robertson pupils are small, irregular pupils that show light-near dissociation, a classic but now uncommon finding associated with neurosyphilis.
What to Bring to Your Visit
Two simple things solve a surprising number of cases. Old photographs - driver's license, passport, family snapshots, or phone selfies - can show whether the pupil difference is new or has been present for years, which immediately changes the level of concern. A complete list of medications and exposures - eye drops, motion-sickness patches, inhalers, migraine medicines, and any contact with plants or chemicals - helps identify pharmacologic causes that mimic neurological disease.
Frequently Asked Questions
Can a normal, healthy person have unequal pupils?
Yes. Physiologic anisocoria is common, usually small (about a millimeter or less), stays roughly the same in light and dark, and comes with normal pupil reactions and no other symptoms. It needs no treatment.
Why does my doctor dim the lights and then shine a flashlight?
Because the lighting tells them which pupil is abnormal. A difference that is larger in bright light means the bigger pupil is failing to constrict; a difference that is larger in the dark means the smaller pupil is failing to dilate. That single observation steers the whole evaluation.
When are unequal pupils an emergency?
The most important emergency pattern is a newly dilated pupil with a droopy eyelid and double vision, or with a sudden severe headache - call 911 or go to an emergency department, because this can signal an aneurysm. Unequal pupils after head trauma, or with weakness, slurred speech, fainting, or confusion, also need emergency care. A new, painful smaller pupil with neck pain should be evaluated promptly as well.
My pupils have always been a little different. Should I worry?
If the difference is longstanding (old photos confirm it), unchanged in different lighting, and not accompanied by a droopy lid, double vision, pain, or vision change, it is very likely physiologic and harmless. New or changing anisocoria, or anisocoria with any of those warning signs, is what warrants evaluation.
References
- American Academy of Ophthalmology. Anisocoria. EyeWiki.
Medical Disclaimer: This information is for educational purposes only and does not replace professional medical advice.