Microvascular Decompression
The Jannetta operation for hemifacial spasm: a neurosurgeon cushions the artery that is pulsing against the facial nerve at the brainstem. It targets the cause rather than masking the twitch, and in well-selected patients the relief can be lasting.
Microvascular decompression (MVD), commonly called the Jannetta procedure after the neurosurgeon who established it, is the one treatment for hemifacial spasm that addresses the cause rather than the twitch. Botulinum toxin quiets the muscles that are misfiring; MVD goes to the brainstem and removes the irritation that is making the nerve fire in the first place. Because it is open intracranial surgery, it is not offered lightly, and the entire conversation turns on whether a patient's spasm is severe enough, and their health robust enough, to justify a craniotomy over an indefinite series of injections.
Key takeaways
- It treats the mechanism, not the symptom - a cushion separates the offending vessel from the facial nerve where the spasm originates
- The realistic alternative is lifelong botulinum toxin, repeated every few months; MVD is the option that can end treatment altogether
- Published surgical series report durable relief in roughly 85 to 90 percent of carefully selected patients, sometimes after a delay of weeks to months
- The signature serious risk is hearing loss on the operated side, because the hearing nerve sits next to the surgical field; facial weakness, cerebrospinal fluid leak, and very rarely stroke or death are the other risks to weigh
- Candidate selection is strict - clear diagnosis, disabling spasm, good general health, and imaging that fits
Questions about your diagnosis? Contact our office
Why a Blood Vessel Causes the Twitch
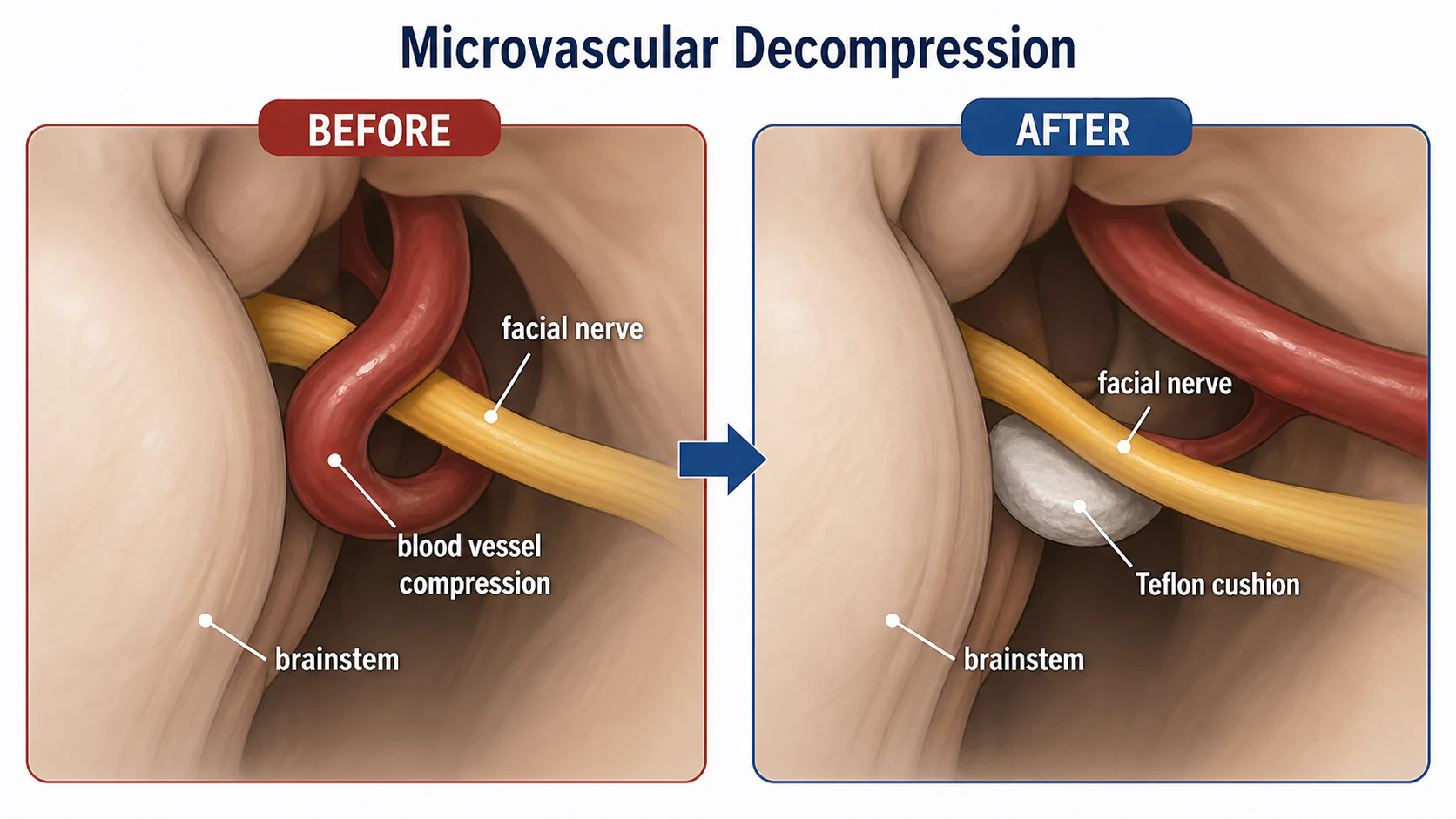
Hemifacial spasm almost always begins at one specific spot: the root exit zone of the facial nerve, the short segment where the nerve leaves the brainstem before it acquires its tougher insulating sheath. There, the nerve is unusually vulnerable, and a nearby artery - most often a loop of the anterior inferior cerebellar artery, the posterior inferior cerebellar artery, or the vertebral artery - can come to rest against it. With every heartbeat the vessel pulses, and over years that repetitive pressure is thought to wear on the nerve's insulation and set up abnormal, self-perpetuating firing. The result is the involuntary contraction that typically starts around the eye and gradually spreads down the same side of the face.
MVD is built directly on that mechanism. The surgeon identifies the offending vessel, lifts it off the nerve, and interposes a soft, inert pad - commonly shredded Teflon felt - so the pulsation can no longer reach the nerve. Nothing is cut or removed from the nerve itself; the nerve is simply relieved of the thing irritating it, and given time, the abnormal firing often settles.
Botulinum Toxin for Life, or One Operation?
For most people, botulinum toxin injections are the first and often the only treatment they ever need. They are done in the office, carry a low procedural burden, and reliably soften the spasm. Their limitation is structural: the toxin wears off, so the injections must be repeated roughly every three to four months, essentially indefinitely, and some patients find the effect fades or becomes less even over years.
MVD enters the conversation when that arrangement stops working for someone. Good candidates generally share several features:
- A confident diagnosis of hemifacial spasm, not a mimicking condition such as blepharospasm or a facial tic
- Spasm severe enough to be genuinely disabling - affecting vision when the eye is squeezed shut, social comfort, or daily function
- Injections that are no longer adequate, are not well tolerated, or that the patient does not want to continue for the rest of their life
- General health sufficient for general anesthesia and intracranial surgery
- An MRI/MRA that shows a vessel in contact with the nerve, which supports the plan (though imaging is a guide, not a substitute for what the surgeon finds in the operating room)
A younger, otherwise healthy patient facing potentially decades of injections is a very different decision than an older patient with heart or lung disease, for whom continued injections are usually the wiser course.
What the Published Series Actually Show
Across large published surgical series, MVD produces lasting resolution of hemifacial spasm in the range of 85 to 90 percent of well-selected patients. Two nuances matter when reading those numbers. First, relief is not always immediate: a meaningful fraction of patients leave the hospital still twitching and then watch the spasm fade over the following weeks to months - the so-called delayed resolution, thought to reflect the nerve slowly recovering after the pulsation is removed. Second, a small percentage have incomplete relief or a later recurrence, sometimes from the cushion shifting or a second vessel that was not addressed. These figures come from specialized centers, and outcomes depend heavily on accurate diagnosis and surgical experience.
Inside the Operation
MVD is performed under general anesthesia and usually takes a few hours. The surgeon makes a small incision behind the ear and removes a coin-sized piece of bone - a retrosigmoid craniotomy - to reach the cerebellopontine angle, the fluid-filled corner where the facial and hearing nerves emerge from the brainstem. The cerebellum is gently retracted, the offending vessel is found, and the cushion is placed. Throughout, the team typically monitors the hearing nerve with brainstem auditory evoked potentials, watching for any change that would prompt them to adjust their technique before damage occurs.
Afterward, patients are watched closely, sometimes in an intensive care setting overnight, with a typical hospital stay of about two to four days. Early on, incisional soreness, fatigue, headache, and some unsteadiness or imbalance are common and usually settle over the following weeks.
The Risk That Deserves the Most Attention
Like any intracranial operation, MVD carries the usual risks of anesthesia along with bleeding and infection. The complication most specific to it is hearing loss on the operated side, because the surgical corridor runs right past the hearing nerve, which is why hearing is monitored during the operation and tested beforehand; when it happens, it can be permanent. The main lasting risks to weigh are hearing loss, facial weakness, and cerebrospinal fluid leak or infection, with stroke or death being very rare. Most facial weakness after surgery is temporary and recovers, while permanent facial weakness is uncommon. Overall, serious long-term complications fall in the low single-digit percentages. These are the trade-offs weighed against the prospect of never needing another injection.
Recovery and the Long View
Most people are back to light activity within a couple of weeks and to fuller activity over four to six weeks, guided by the surgical team. Because relief may be immediate or delayed, surgeons generally counsel patients not to judge the result in the first days. When MVD succeeds, it tends to stay successful, and many patients never require treatment for spasm again.
MVD Versus Botulinum Toxin at a Glance
| Microvascular decompression | Botulinum toxin injections |
|---|---|
| Targets the underlying vascular compression | Relaxes the overactive muscles, not the cause |
| Aims for a one-time, potentially permanent cure | Ongoing treatment, repeated every 3 to 4 months |
| Intracranial surgery: hearing loss, facial weakness, CSF leak, rare stroke or death | Office procedure: temporary local weakness, occasional ptosis or dry eye |
| Hospital stay and weeks of recovery | Same-day, minimal downtime |
| Best for disabling spasm in healthy candidates | Suits most patients, including those who cannot have surgery |
Frequently Asked Questions
Will the spasm stop the moment I wake up from surgery?
Sometimes, but not always. Some patients notice the twitching is gone immediately; others continue to spasm for weeks or even a few months before it gradually resolves as the nerve recovers. Your surgeon will usually ask you to give it time before judging whether the operation worked.
If I have MVD, can I stop botulinum toxin entirely?
That is the goal, and for most patients who do well, yes. Because the result can take time to appear, your team may keep injections available during the early recovery window if the spasm is still bothersome, then taper them off as the surgical benefit emerges.
Does the Teflon cushion ever need to be replaced?
It is meant to be permanent and is not routinely replaced. In the small number of patients whose spasm returns, imaging and clinical judgment determine whether a second operation makes sense - sometimes the cushion has shifted or another vessel is involved.
Why do I need a hearing test before and after?
The hearing nerve runs alongside the surgical field, so hearing is the function most at risk. A baseline test documents your hearing before surgery, monitoring during the operation helps protect it, and a follow-up test confirms it afterward.
References
- MedlinePlus. Trigeminal Neuralgia.
- American Academy of Ophthalmology EyeWiki. Hemifacial Spasm.
Medical Disclaimer: This information is for educational purposes only and does not replace professional medical advice. Decisions about neurosurgery for hemifacial spasm should be made with a neurosurgeon and your neuro-ophthalmologist.