Skew Deviation
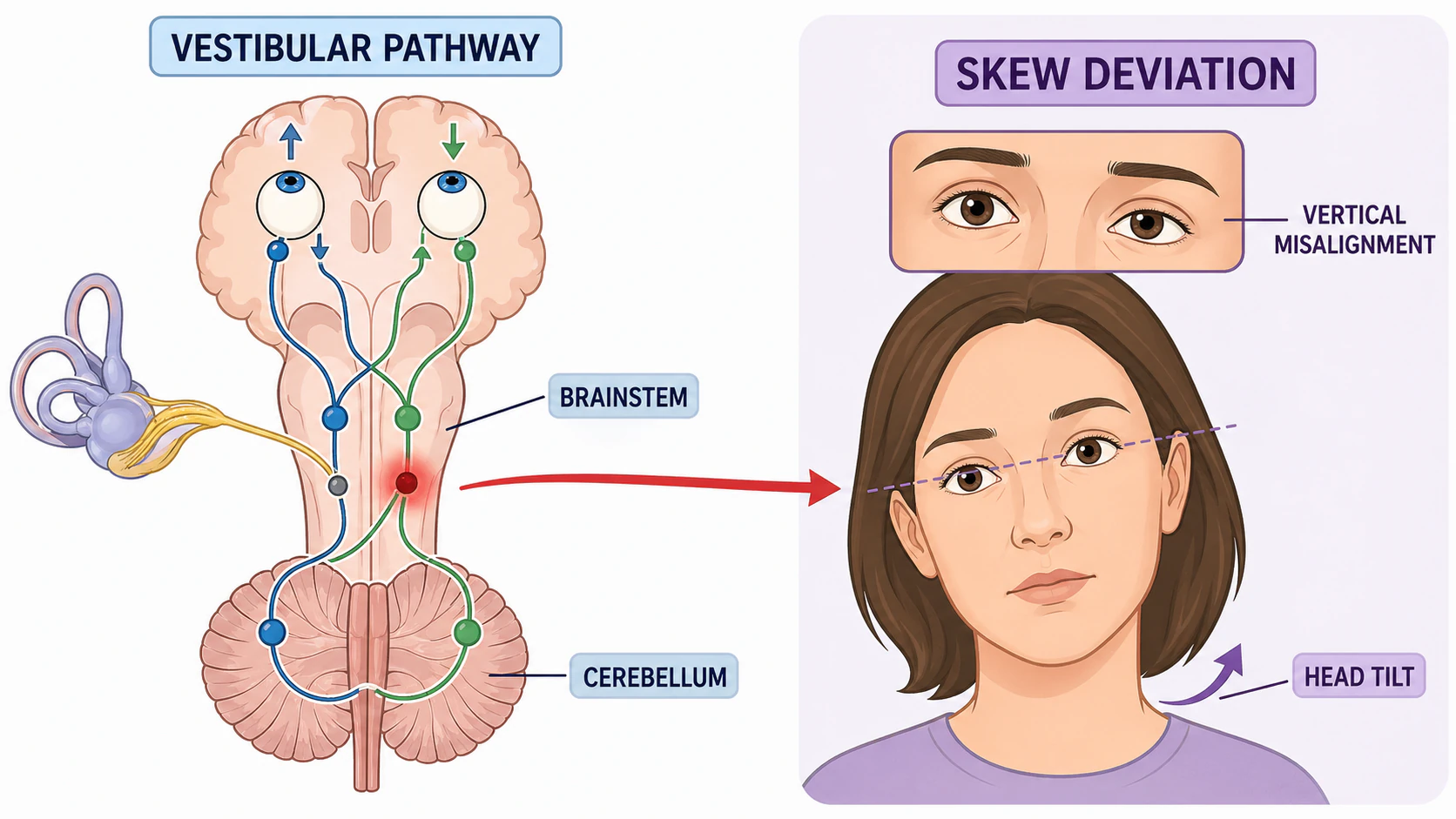
Vertical eye misalignment caused by brainstem or cerebellar lesions. The eyes are misaligned up and down rather than side to side, and the pattern does not follow any single eye muscle.
Skew deviation is a vertical or oblique misalignment of the eyes caused by an imbalance in the central pathways that keep the eyes level - most often in the brainstem or cerebellum. Unlike other causes of vertical double vision, the misalignment in skew does not follow the pattern of any single eye muscle or cranial nerve. That is precisely what makes it an important sign: when it is present, the problem usually lies in the brain or the vestibular pathways rather than in the eye muscles themselves.
Key takeaways
- Skew deviation is a central sign - it points to the brainstem or cerebellum, not to an eye muscle or cranial nerve
- The pattern does not match a single muscle, which is what separates it from a fourth nerve palsy
- It is often part of the ocular tilt reaction - vertical misalignment combined with a head tilt and torsion of the eyes
- In acute vertigo, the test of skew is one part of the HINTS exam used to distinguish stroke from inner-ear causes
- A new skew usually prompts an MRI of the brain, because the differential includes stroke, demyelination, and other posterior-fossa lesions
Questions about your diagnosis? Contact our office
How the Vestibular System Keeps the Eyes Level
The vestibular system holds the eyes level even as the head tilts and moves. Gravity-sensing organs in the inner ear (the otoliths, or utricles) send signals up through the brainstem to the eye muscles, continuously adjusting eye position so the visual world stays upright. When this otolith-ocular pathway is damaged anywhere along its course, the balance between the two sides is lost and one eye drifts up while the other drifts down. The result is a vertical misalignment that has nothing to do with a weak muscle - the muscles are working, but the instructions reaching them are skewed.
What Skew Deviation Looks Like
On examination the doctor sees a vertical difference in eye position: one eye sits higher (a hypertropia) and the other lower (a hypotropia). The gap may be small - a few prism diopters - or large enough that the patient reports one image floating above the other. The misalignment is best brought out by the alternate cover test: as the cover is moved from one eye to the other, the newly uncovered eye makes a corrective vertical movement to take up fixation.
What flags the deviation as a skew - rather than another cause of vertical misalignment - is that it does not behave like a single weak muscle. A right superior oblique palsy (a right fourth nerve palsy) follows a stereotyped pattern: the right eye is higher, the deviation worsens on left gaze and on right head tilt, and improves on right gaze and left head tilt. Skew deviation usually breaks that pattern. The vertical difference may be roughly the same in all directions of gaze, or it may change in a way that does not implicate any one muscle.
Associated symptoms
Because skew arises from brainstem or cerebellar problems, it often travels with other signs:
- Vertical double vision - one image above the other, present in most or all directions of gaze
- Dizziness, vertigo, or imbalance
- A head tilt the patient may not be aware of
- Oscillopsia - the sense that the world is bobbing or shimmering
- Other brainstem signs such as weakness, numbness, slurred speech, or trouble swallowing
The Ocular Tilt Reaction
Skew deviation is frequently one piece of a three-part syndrome called the ocular tilt reaction (OTR):
- Skew deviation - the vertical misalignment itself
- Head tilt - the head tips toward one shoulder; the direction depends on where the lesion sits
- Ocular torsion - both eyes rotate around the line of sight; in skew, the lower eye is typically excyclotorted (rolled outward) and the higher eye incyclotorted (rolled inward)
The whole reaction reflects a disturbance of the otolith-ocular pathway carrying gravity information from the inner-ear utricles up through the brainstem. The direction of the tilt has localizing value, which is unusual and useful at the bedside:
- Ipsiversive OTR (lesions in the medulla, lower pons, or the peripheral vestibular organ) - the head tilt and the lower eye are toward the side of the lesion
- Contraversive OTR (lesions above the pontomedullary crossing, into the mid-pons and midbrain) - the head tilt and the lower eye are away from the side of the lesion
This is one of the few neuro-ophthalmic signs that helps pinpoint a level within the brainstem from the examination alone.
Skew Deviation Versus Fourth Nerve Palsy
Distinguishing skew from a fourth nerve palsy is the differential the doctor weighs whenever a vertical misalignment turns up, because it changes the workup completely - a skew sends the evaluation toward the brain, while an isolated fourth nerve palsy is often simply observed.
| Feature | Skew deviation | Fourth nerve palsy |
|---|---|---|
| Location of lesion | Brainstem / cerebellum | Fourth cranial nerve |
| Parks 3-step test | Does not match a single muscle | Matches one superior oblique |
| Misalignment across gaze | Often relatively constant | Worsens on contralateral gaze |
| Bielschowsky head-tilt test | No clear improvement with one head tilt | Improves with head tilt to the opposite side |
| Ocular torsion direction | Higher eye intorts; lower eye extorts | Higher eye extorts |
| Other neurological signs | Often present (vertigo, ataxia, weakness) | Usually isolated |
| Imaging | MRI often indicated for a new skew | Often observed if isolated and stable |
The torsional pattern is one of the most specific bedside clues. In a fourth nerve palsy, the higher eye is excyclotorted (its top rolls outward), because the paretic superior oblique normally intorts the eye. In skew deviation as part of the ocular tilt reaction, it is the opposite: the higher eye intorts and the lower eye extorts. Put simply - in skew, the lower eye extorts; in a fourth nerve palsy, the higher eye extorts.
Skew Deviation in Acute Vertigo: the HINTS Exam
When someone arrives with sudden, continuous vertigo, the urgent question is whether the cause is peripheral (the inner ear - usually benign) or central (a brainstem or cerebellar stroke - an emergency). The HINTS exam combines three bedside findings to answer it:
- Head Impulse test - an abnormal (catch-up) response points to a peripheral cause
- Nystagmus - direction-changing nystagmus is a central sign
- Test of Skew - the presence of skew deviation is a central sign
Among patients with the acute vestibular syndrome, the HINTS exam - performed by clinicians trained in its interpretation - has been shown to be more sensitive than early diffusion-weighted MRI (in the first 24-48 hours after onset) for detecting posterior-circulation stroke; later MRI catches up. A clear skew in this setting is especially worrying and prompts urgent imaging and stroke evaluation, though small ocular tilt reactions can occasionally occur with peripheral vestibular disease and must be read alongside the rest of the exam.
Sudden vertical double vision with severe dizziness, imbalance, slurred speech, facial droop, or limb weakness can be a brainstem or cerebellar stroke. Call 911 immediately. A stroke at the back of the brain can cause these symptoms with little else to warn you, so do not wait to see if it passes and do not drive yourself.
What Causes Skew Deviation
The differential mirrors what can injure the brainstem and cerebellum:
- Posterior-circulation stroke - including lateral medullary (Wallenberg) syndrome, AICA infarcts, and cerebellar strokes
- Multiple sclerosis with brainstem demyelinating plaques, a common cause in younger adults
- Brainstem or cerebellar tumors
- Intracranial hemorrhage
- Traumatic brain injury, especially with brainstem involvement
- Wernicke encephalopathy - thiamine deficiency; the eye signs are more often a sixth-nerve palsy and nystagmus, but skew can occur as part of the broader brainstem dysfunction
- Hydrocephalus and chronically raised intracranial pressure, which can produce a skew or pattern misalignment
- Cerebellopontine-angle and brainstem masses - vestibular schwannoma, meningioma, and others, sometimes appearing after surgery to remove them
- Internuclear ophthalmoplegia, which is sometimes accompanied by a small skew
How the Finding Is Confirmed
Cover testing
The alternate cover test is the standard bedside method. The examiner covers one eye, then quickly shifts the cover to the other while watching the newly uncovered eye for a vertical refixation movement. A vertical correction that persists across gaze directions - and that does not match a single-muscle pattern - supports skew.
Maddox rod and double-Maddox rod
A red Maddox rod turns a point of light into a line, letting the doctor measure vertical and torsional misalignment precisely. With the double-Maddox rod test - a differently colored rod over each eye, which the patient rotates until both lines look level - any cyclotorsion can be quantified, which is particularly helpful for telling a skew apart from a fourth nerve palsy.
Upright-supine test
This bedside maneuver is fairly specific for skew. The vertical misalignment is measured first with the patient sitting upright, then again lying flat. Skew deviations typically shrink substantially - often by half or more - when the patient lies down, because gravity-dependent otolith input falls; a fourth nerve palsy stays roughly the same. New vertical misalignment with neurologic features usually warrants neurologic evaluation and imaging, described below.
Imaging and vestibular testing
An MRI of the brain, focused on the brainstem and cerebellum, is the central test for a new or acquired skew, looking for stroke, MS plaques, tumor, or hemorrhage. Vestibular testing may be added when vertigo or imbalance is prominent, to help separate a peripheral from a central cause.
Treatment and Outlook
A new skew deviation is treated first as a sign that needs an explanation, not as a problem to be patched in isolation.
- Treat the underlying cause - stroke management, MS treatment, tumor care, or correction of any treatable condition. As the lesion stabilizes, the skew itself often improves over weeks to months.
- Prism glasses can compensate for a stable residual misalignment and relieve double vision.
- Patching one eye is a simple temporary measure to eliminate diplopia while the cause is being addressed.
- Strabismus surgery is occasionally considered for a stable, long-standing skew that prisms cannot manage.
Prognosis is variable and tied to the cause: post-stroke and post-demyelination skews often recover meaningfully, while some persist and are managed optically.
Frequently Asked Questions
How is skew deviation different from other causes of double vision?
Skew is a specific vertical misalignment driven by disordered vestibular control of eye position in the brainstem or cerebellum, rather than by a weak muscle or a single cranial nerve. Unlike a fourth nerve palsy, its pattern does not match one eye muscle - and that distinction matters, because skew usually points to a problem inside the brain.
Does skew deviation mean I had a stroke?
Not necessarily, but stroke is one of the most important causes to rule out, especially when the skew comes on suddenly or alongside vertigo, double vision, or weakness. That is why imaging is commonly part of the workup, and why sudden onset with neurologic symptoms is treated as an emergency.
Why did the doctor have me lie down during the exam?
The upright-supine test helps separate skew from a fourth nerve palsy. A skew deviation usually decreases substantially when you lie flat, because the gravity signals that drive it are reduced, while a fourth nerve palsy stays about the same.
Will my double vision go away?
Often it improves, particularly when the underlying cause recovers or is treated - many skews after stroke or a demyelinating attack settle over weeks to months. When a stable misalignment remains, prism glasses, or occasionally surgery, can manage it well.
Is skew the same as crossed eyes?
No. "Crossed eyes" in everyday speech usually means esotropia - eyes turning inward. Skew is specifically a vertical or oblique misalignment caused by a central nervous system problem. Both are forms of strabismus, but the cause and the workup are different.
References
- Brodsky MC, Donahue SP, Vaphiades M, Brandt T. Skew deviation revisited. Surv Ophthalmol. 2006;51(2):105-128.
- Wong AM. Understanding skew deviation and a new clinical test to differentiate it from trochlear nerve palsy. J AAPOS. 2010;14(1):61-67.
- Kattah JC, Talkad AV, Wang DZ, et al. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI. Stroke. 2009;40(11):3504-3510.
- Brandt T, Dieterich M. Skew deviation with ocular torsion: a vestibular brainstem sign of topographic diagnostic value. Ann Neurol. 1993;33(5):528-534.
- American Academy of Ophthalmology EyeWiki. Skew Deviation.
Medical Disclaimer: This information is for educational purposes only and does not replace professional medical advice, diagnosis, or treatment. If you have concerns about double vision or any symptoms, please consult a qualified healthcare provider.