Optic Atrophy
Pallor of the optic disc that marks the loss of optic nerve fibers. Atrophy is an endpoint, not a diagnosis - the central task is hunting down the cause and stopping any damage that is still treatable.
Optic atrophy is the pale appearance the optic disc takes on after optic nerve fibers have been damaged and lost. The healthy disc looks pink-orange because it is densely packed with nerve fibers and tiny blood vessels; when those fibers die, the tissue thins and the disc turns pale. The single most important idea about optic atrophy is that it is a sign, not a diagnosis. It tells you that the nerve has been injured at some point - but it says nothing, by itself, about what did the injuring. The clinical work that follows a finding of optic atrophy is a focused hunt for the cause, driven by one question above all: is any part of this process still active and still treatable?
Key takeaways
- Optic atrophy is the end result of nerve fiber loss, not a disease in its own right
- The fibers that are already lost do not grow back, so the pallor itself is permanent
- The pattern of pallor and the rest of the exam often point toward the underlying cause
- Distinguishing glaucomatous cupping from non-glaucomatous pallor changes the entire workup
- The reason to investigate even old-looking atrophy is to find anything still ongoing - compression, inflammation, a nutritional deficiency, or an inherited disease
Questions about your diagnosis? Contact our office
What It Looks Like
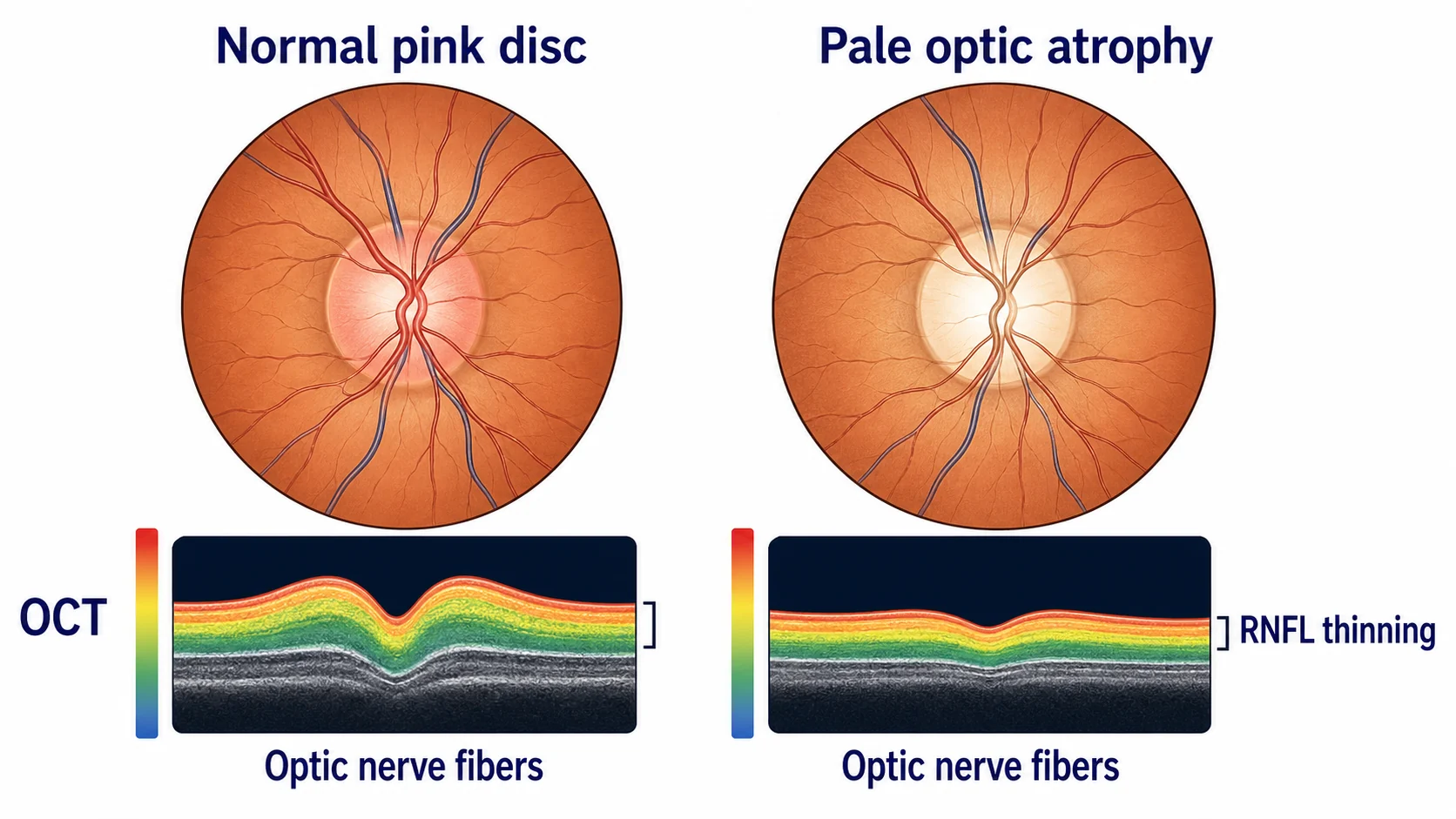
On examination the disc appears pale rather than its normal pink-orange, the small surface blood vessels are reduced in number, and the change may be complete (the whole disc) or segmental (only part of it). OCT imaging confirms and quantifies the loss by showing thinning of the retinal nerve fiber layer around the disc and of the ganglion cell layer in the macula. A relative afferent pupillary defect is often present when one eye is more affected than the other, and visual function - acuity, color, and field - is reduced in proportion to how much of the nerve has been lost.
A Sign, Not a Diagnosis
Because optic atrophy is the common endpoint of many different injuries, two patients with identically pale discs can have completely different problems - one a resolved episode of optic neuritis years ago, another a slowly enlarging tumor pressing on the nerve right now. The pallor looks the same; the urgency could not be more different. This is why "optic atrophy" is never a satisfying final answer. The clinically useful answer names the cause and states whether it is finished or ongoing.
What the Pattern of Pallor Can Suggest
The way the disc is pale, combined with how the visual field has been lost, often narrows the field of suspects:
- Temporal (side-facing) pallor affecting the papillomacular bundle is characteristic of prior optic neuritis, and of toxic, nutritional, and several hereditary optic neuropathies.
- "Band" or "bow-tie" atrophy - horizontal pallor across the disc - suggests loss of fibers from the nasal retina, the pattern produced by chiasmal compression causing a temporal field defect, and is a clue to look for a lesion at the optic chiasm.
- Diffuse pallor of the whole disc is the least specific and fits many causes.
- Sector pallor can follow a branch vascular event or segmental injury.
These patterns are pointers, not proof, but they help direct imaging and testing efficiently.
The Cause Hunt
Causes are usually grouped by mechanism, and the grouping itself guides the workup:
- Inflammatory / demyelinating - prior optic neuritis, or relapses of neuromyelitis optica (NMO), which can leave severe atrophy.
- Vascular - ischemic optic neuropathy, including the arteritic form caused by giant cell arteritis, which must be considered urgently in older adults because the fellow eye is at risk.
- Compressive - a pituitary tumor, an optic nerve sheath meningioma, or other masses; compression is the category most worth catching because relieving it can sometimes preserve remaining vision.
- Hereditary - Leber hereditary optic neuropathy (LHON) and dominant optic atrophy, which often present with bilateral, symmetric, often temporal pallor.
- Long-standing swelling - chronic papilledema that eventually damages the nerve.
- Toxic and nutritional - deficiencies (notably vitamin B12 and folate) and exposures (including certain drugs, tobacco, and excessive alcohol), which are important precisely because they are treatable and often bilateral.
- Other - trauma, glaucoma, and developmental or neonatal injury; a physician-authored case summary illustrates Wallerian degeneration after neonatal intracranial hemorrhage.
Pallor Versus Cupping: Two Different Stories
A practical and important distinction is between glaucomatous and non-glaucomatous optic nerve damage, because they look different and mean different things. In glaucoma the hallmark is cupping - the central depression of the disc enlarges and the neuroretinal rim thins or notches - typically with relatively preserved rim color until late. In most non-glaucomatous causes the dominant change is pallor that exceeds the degree of cupping: the disc is distinctly pale without the deep, expanded cup of glaucoma. When pallor is out of proportion to cupping, the evaluation shifts away from a pure pressure problem and toward a compressive, inflammatory, ischemic, hereditary, or toxic cause - frequently prompting neuroimaging. Getting this distinction right is what keeps a treatable tumor or a giant cell arteritis from being mislabeled as glaucoma.
The Workup
The investigation is tailored to the suspected mechanism, but commonly includes:
- A detailed history - speed of onset, pain, prior episodes, family history, medications, diet, and alcohol or tobacco use
- Visual field testing to map the pattern of loss, which itself localizes the injury
- OCT to quantify nerve fiber and ganglion cell loss and to follow it over time
- Color vision testing, since color is often affected early and disproportionately in optic nerve disease
- MRI of the brain and orbits to look for compression, inflammation, or a chiasmal lesion
- Blood tests as indicated - inflammatory markers (urgently, if giant cell arteritis is a concern), B12 and folate, and targeted antibody or genetic testing when an inflammatory or inherited cause is suspected
What It Means for Your Vision
Once optic atrophy is established, the nerve fibers that have been lost will not regenerate, and any vision loss they caused is generally permanent. That sounds bleak, but it is not the whole story, and it is why the workup is still worthwhile:
- If part of the picture is reversible - residual swelling, active inflammation, or compression that can be relieved - treating it can protect or even recover some function.
- Finding a systemic or treatable cause (a nutritional deficiency, an inflammatory disease, an inherited condition with implications for family members) changes management well beyond the eye.
- Low vision rehabilitation helps make the most of remaining sight, and our guide on adapting to vision loss offers practical support.
The goal, in short, is to preserve every fiber that can still be saved and to ensure that nothing ongoing or systemic is missed.
Frequently Asked Questions
Is optic atrophy the same thing as optic neuritis?
No. Optic neuritis is one possible cause - an episode of inflammation of the nerve. Optic atrophy is the pale, thinned appearance that can be left behind afterward, and it can follow inflammation and many other injuries.
Can optic atrophy improve or be reversed?
The lost fibers themselves do not regrow, so established atrophy is permanent. Vision can still improve if there is reversible swelling, inflammation, or compression alongside the atrophy, which is one reason the cause is always worth investigating.
Why do I need an MRI and blood tests if the damage is already done?
Because the central question is not what already happened but whether anything is still happening. Imaging, fields, OCT, and targeted blood work separate old, stable damage from ongoing compression, active inflammation, a nutritional deficiency, or an inherited disease - some of which are treatable and some of which matter for your family.
If both my optic nerves are pale, does that change things?
Often, yes. Bilateral, symmetric atrophy raises the likelihood of toxic, nutritional, hereditary, or compressive (chiasmal) causes, and it points the workup toward blood tests, dietary and exposure history, genetic evaluation, and imaging of the chiasm.
References
- American Academy of Ophthalmology. Optic Atrophy. EyeWiki.
- Osborne NN, et al. Optic nerve and neuroprotection strategies. Eye. 2004;18(11):1075-1084.
Medical Disclaimer: This information is for educational purposes only and does not replace professional medical advice.