Orbital Decompression Surgery
Surgery that enlarges the bony eye socket in thyroid eye disease. It is urgent and sight-saving when swollen tissue strangles the optic nerve, and rehabilitative when the goal is to reverse bulging and protect the cornea.
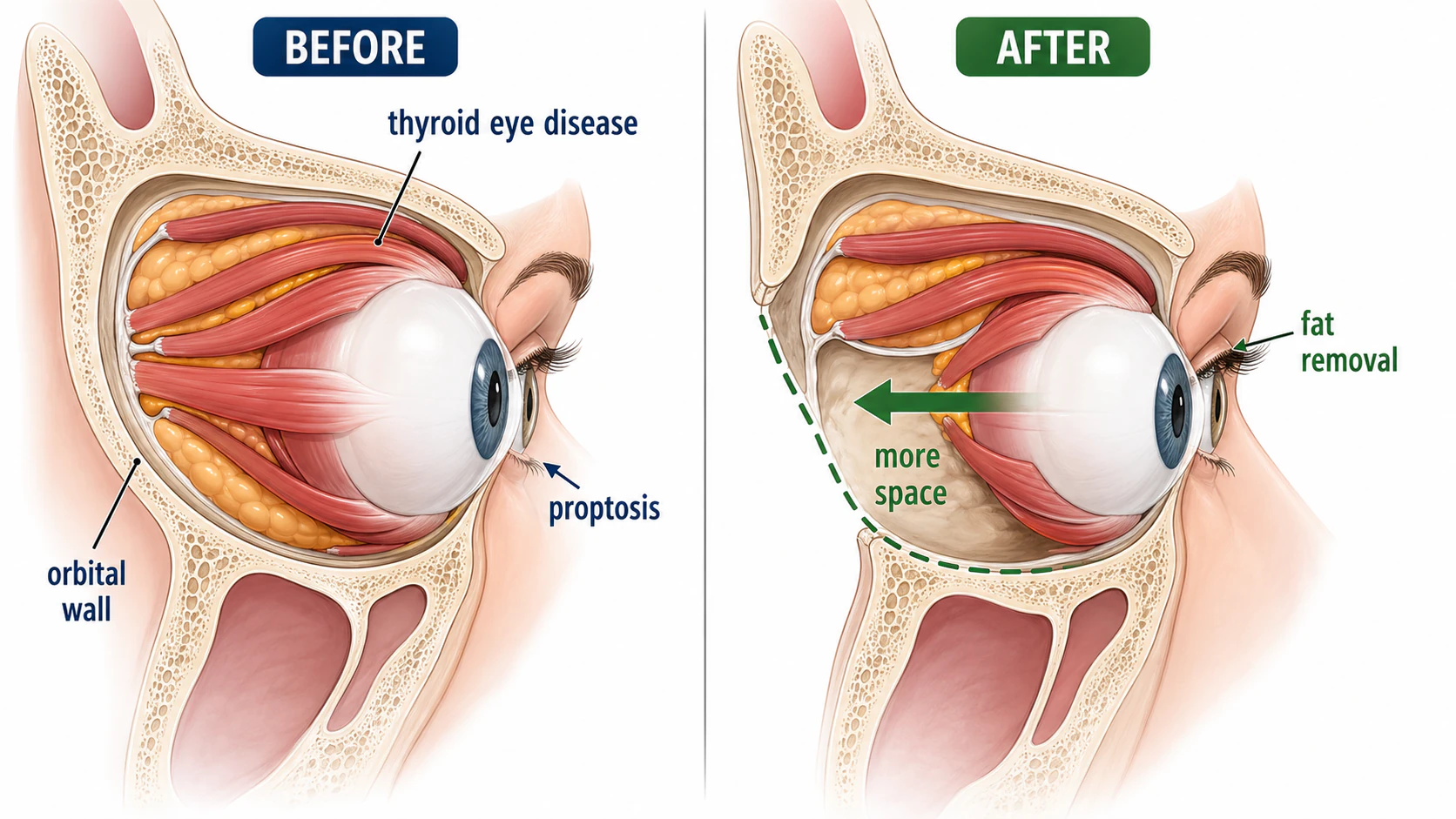
Orbital decompression enlarges the space inside the bony eye socket. It exists because of a basic mechanical problem in thyroid eye disease: the orbit is a rigid cone of bone with a fixed volume, and when the eye muscles and fat inside it swell, the contents have nowhere to go but forward. Mild swelling pushes the eye outward, producing the bulging look of proptosis. Severe swelling at the back of the orbit can do something far more dangerous - crush the optic nerve where it exits. Decompression removes part of the bony wall, fat, or both, so the swollen tissue can spill into the space next door instead of crowding the eye and nerve.
Key takeaways
- The orbit is a closed bony box - when its contents swell, the eye is pushed forward and the optic nerve can be compressed
- There are two very different reasons to operate: an urgent one (the nerve is being compressed and vision is at risk) and a rehabilitative one (reducing bulging and protecting the cornea once the disease has calmed)
- Surgeons make room by removing bony walls, orbital fat, or both - more walls usually means more reduction but a higher chance of new double vision
- Sequence matters: when several operations are needed, decompression comes first, then eye-muscle surgery, then eyelids
- New or worse double vision is the main trade-off to understand before consenting
Questions about your diagnosis? Contact our office
Compressive optic neuropathy is a sight-threatening emergency. If you have thyroid eye disease and notice your vision dimming, colors looking washed out or faded, or a new blind area, contact your ophthalmologist or go to the emergency department the same day. Optic nerve compression can cause permanent vision loss if it is not relieved quickly, and decompression may need to be done urgently.
Why the Orbit Runs Out of Room
The orbit holds the eye, its six muscles, the optic nerve, and a cushion of fat, all packed into a bony socket whose walls do not move. In thyroid eye disease, autoimmune inflammation makes the muscles and fat enlarge. Because the bone cannot expand, the rising pressure follows the path of least resistance, which is forward - so the eye protrudes. But the back of the orbit, the apex, is a tight funnel where the optic nerve passes through a narrow channel. When swollen muscles bulk up at the apex, they can compress the nerve directly. This is compressive (dysthyroid) optic neuropathy, and unlike the cosmetic and comfort problems of bulging, it threatens sight. Decompression is the mechanical answer to a mechanical problem: take down a wall, and the pressure has somewhere to vent.
Two Very Different Reasons to Operate
The same operation serves two distinct purposes, and the urgency could not be more different.
Urgent: saving the optic nerve
When the nerve is being compressed - signaled by falling vision, loss of color vision, a new visual field defect, or a relative afferent pupillary defect on exam - the situation is time-sensitive. High-dose intravenous steroids are often started first to reduce inflammation quickly, but if the nerve does not recover or the compression is severe, decompression is done to physically relieve the pressure. Here the goal is not appearance at all; it is to keep temporary, reversible pressure from becoming permanent vision loss.
Rehabilitative: undoing the damage once the disease is quiet
Most decompressions are not emergencies. They are done after the active inflammatory phase has burned out and the disease is stable, to address what it left behind: disfiguring proptosis, an eye that no longer closes fully and exposes the cornea to drying and ulceration, and the ache and pressure of a crowded orbit. These operations are planned, elective, and aimed at rehabilitation - restoring a more normal eye position and protecting the ocular surface.
How Surgeons Make Space
There are two levers, often used together.
Bony wall (deep) decompression removes portions of the orbital walls so tissue can herniate into the adjacent sinuses or the temple. The medial wall (into the ethmoid sinus), the floor (into the maxillary sinus), and the lateral wall are the workhorses, used in different combinations. As a rule, the more walls removed, the greater the reduction in proptosis - and the greater the risk of new double vision, because shifting the muscles changes how the two eyes line up. Surgeons sometimes favor a balanced approach (for instance, medial and lateral walls) to reduce that risk.
Fat decompression removes orbital fat rather than bone. It can be enough on its own for milder bulging and tends to carry a lower risk of new double vision than an aggressive multi-wall bony decompression. Fat and bone removal are frequently combined and tailored to how much reduction a particular eye needs.
Why Sequence Matters: Decompression First
Thyroid eye disease often requires more than one operation, and the order is deliberate rather than arbitrary. Decompression changes the position of the eye; eye-muscle surgery changes alignment; eyelid surgery changes how the lids sit. Because each step alters the starting point for the next, doing them out of order would mean re-correcting work already done.
- Orbital decompression first (when needed), to set the eye's position
- Strabismus surgery next, to realign the eyes and address double vision
- Eyelid surgery last, to fine-tune lid position and closure
Skipping ahead - for instance, fixing the eyelids before decompression - risks a result that no longer fits once the eye is moved.
The Trade-Off: New Double Vision
The complication patients most need to understand is new or worsened double vision. Moving the orbital walls can leave the eye muscles pulling at slightly different angles than before, so some patients who saw singly beforehand develop diplopia afterward, and some with existing diplopia find it changes. This is often manageable with prisms or a later strabismus operation, but it is common enough that it must be part of the consent conversation, especially before a large multi-wall decompression. Other possible complications include numbness of the cheek, lip, or teeth; sinus problems, bleeding, or infection; a rare cerebrospinal fluid leak; and under- or over-correction of the eye's position.
Where Teprotumumab Fits
The landscape shifted with teprotumumab (Tepezza), an IGF-1 receptor inhibitor that became the first FDA-approved drug for thyroid eye disease in 2020. Given as a series of infusions during active disease, it can meaningfully reduce proptosis and double vision medically, which in some patients lessens or delays the need for rehabilitative decompression. It is not, however, a universal substitute for surgery: it has its own side effects and cost, response varies, and it does not replace urgent decompression when the optic nerve is acutely threatened. For most patients it is best thought of as another tool that has changed the timing and sometimes the necessity of surgery, decided case by case with the treating team. Our broader thyroid eye disease guide puts these options in context.
Practical Points Before and After
Before an elective operation, thyroid hormone levels should be controlled, the disease should be stable or inactive, and a CT scan is used to map which walls and fat compartments to address; an exophthalmometry measurement documents the baseline proptosis. Stopping smoking genuinely matters - it worsens thyroid eye disease and impairs healing. Afterward, expect swelling, bruising, nasal congestion, and a sensation of pressure; ice and head elevation help in the first days, recovery is measured in weeks, and the eye's final position settles over months. Urgent or multi-wall cases may involve a hospital stay.
Frequently Asked Questions
Is orbital decompression cosmetic surgery?
It can be either, depending on why it is done. When the optic nerve is compressed or the cornea is exposed and at risk, it is functional, sight- and eye-protecting surgery. When the disease is quiet and the aim is to reverse disfiguring bulging, it is rehabilitative - restoring a more normal appearance after an illness, which is different from elective cosmetic surgery on a healthy eye.
Will my eyes look normal again afterward?
Decompression usually reduces the bulging substantially and can dramatically improve appearance, but "normal" varies with how much proptosis there was and how the eyelids and alignment respond. Many patients need the later staged steps - eyelid and sometimes muscle surgery - to complete the rehabilitation.
Can decompression be avoided if I take teprotumumab?
For some patients, yes - reducing proptosis medically can lessen or postpone the need for rehabilitative surgery. But teprotumumab is not right for everyone, responses differ, and it does not substitute for urgent surgery when vision is acutely threatened. The decision is individualized.
What is the warning sign that compression is becoming an emergency?
Dimming vision, colors looking faded or less vivid, or a new dark area in your sight - especially together - are the signals to act on the same day. These changes suggest optic nerve involvement in addition to altered eye position.
References
- American Academy of Ophthalmology EyeWiki. Thyroid Eye Disease.
- National Institute of Diabetes and Digestive and Kidney Diseases. Graves' Disease.
Medical Disclaimer: This information is for educational purposes only and does not replace professional medical advice. Thyroid eye disease management should be coordinated with an oculoplastic surgeon and your endocrinologist.