Visual Field Defects (Patterns)
The shape of a blind area is a map. Whether vision loss is in one eye or both, and whether it respects the vertical or horizontal midline, points to a specific place along the visual pathway - from the retina to the back of the brain.
A visual field defect is a blind or dim area in your range of sight, and its shape is rarely random. The visual pathway runs from each retina, back through the optic nerves, where the nerves cross at the chiasm, and then along the tracts and radiations to the back of the brain - and the fibers are arranged in such an orderly way that damage at each point produces a characteristic pattern. Read correctly, that pattern is a map: it tells the clinician roughly where along the pathway something has gone wrong, often before any scan is done. This page walks the pathway from front to back and shows how each location signs its name.
Key takeaways
- The pattern localizes the lesion - the shape and distribution of the loss point to a specific segment of the visual pathway
- Two questions do most of the work: is the loss in one eye or both, and does it respect a midline?
- Defects respecting the vertical midline sit at or behind the chiasm; the bitemporal pattern marks the chiasm itself
- Homonymous defects - the same side missing in both eyes - lie behind the chiasm, and they become more matched between the eyes the farther back the lesion is
- A new homonymous field loss can be a stroke and needs emergency evaluation
Questions about your diagnosis? Contact our office
Reading a Field Defect Like a Map
Before naming any specific pattern, two questions narrow the location enormously.
One eye or both? A defect in only one eye points in front of the chiasm - to that eye's retina or optic nerve - because before the crossing, each eye's pathway is independent. Once fibers from the two eyes mix at the chiasm and beyond, lesions affect both eyes together.
Does it respect a midline, and which one? The visual world is split down the middle. A defect that stops cleanly at the vertical midline - taking the right half or left half - implicates the chiasm or the pathway behind it, where fibers are sorted by left-versus-right. A defect that respects the horizontal midline - taking a top or bottom half - points instead to the optic nerve or retina, whose fibers are arranged top-versus-bottom. Those two dividing lines are the single most useful clue in the whole exercise.
Before the Chiasm: One Eye at a Time
Damage to a single retina or optic nerve produces a defect in that eye alone.
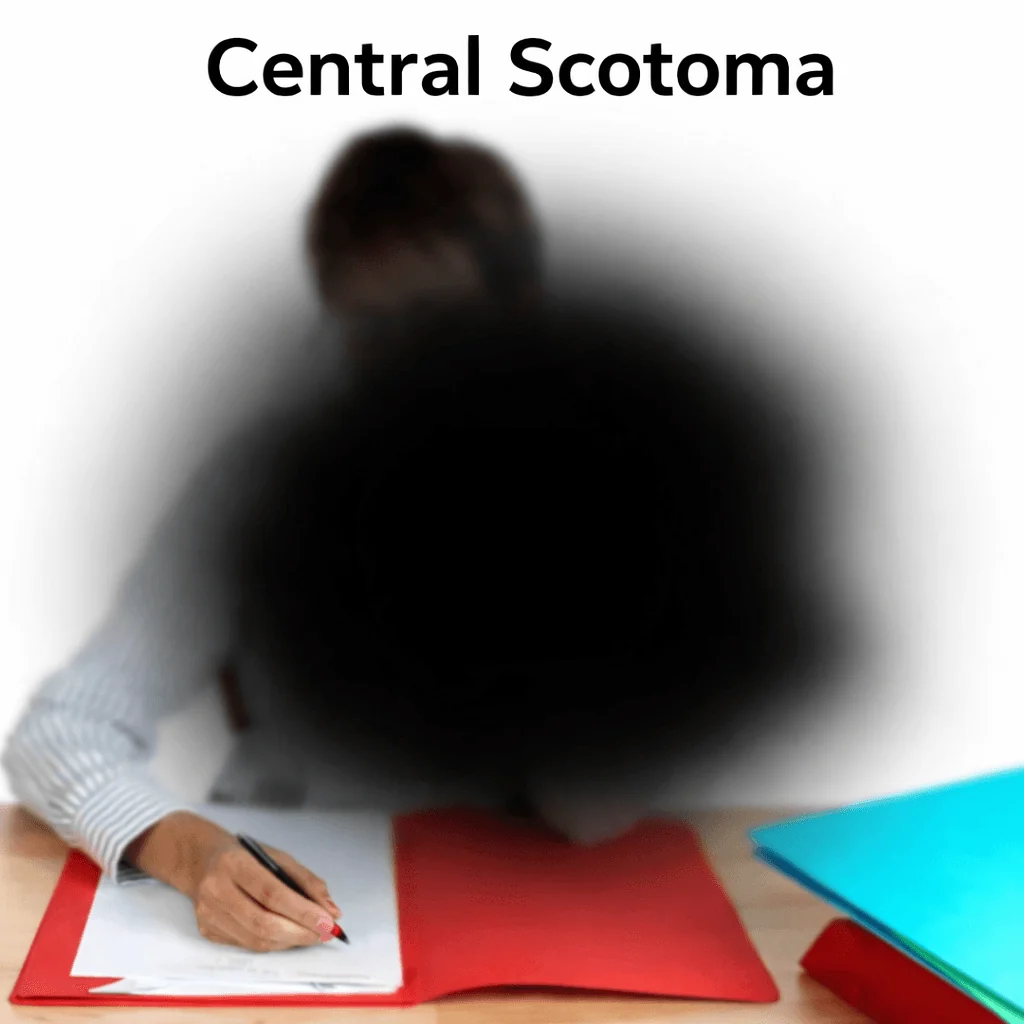
- Central scotoma - a blind or blurred patch right in the middle of vision, wrecking reading and fine detail. It points to the optic nerve, as in optic neuritis, or to the macula, as in macular degeneration. Because nerve and macula can look similar on a field test, an OCT and a dilated retinal exam help separate them.
- Altitudinal defect - loss of the entire top or bottom half of one eye's field, respecting the horizontal midline. This is the signature of ischemic optic neuropathy and of a branch retinal artery occlusion, reflecting the blood supply to the upper or lower nerve or retina.
- Arcuate defect - an arc curving out from the blind spot, following the nerve fiber bundles. It is classic for glaucoma.
- Generalized constriction - the peripheral field closing in all around, seen in advanced glaucoma, some retinal diseases, and chronic papilledema.
A single-eye optic nerve lesion is often accompanied by a relative afferent pupillary defect on exam, another sign the problem sits in front of the chiasm.
At the Chiasm: The Bitemporal Signature
The optic chiasm is where fibers from the nasal (inner) half of each retina cross to the other side. Those nasal fibers carry the temporal (outer) half of each eye's field. A lesion pressing on the center of the chiasm - most often a pituitary tumor growing upward - strikes exactly these crossing fibers, knocking out the outer field of both eyes.
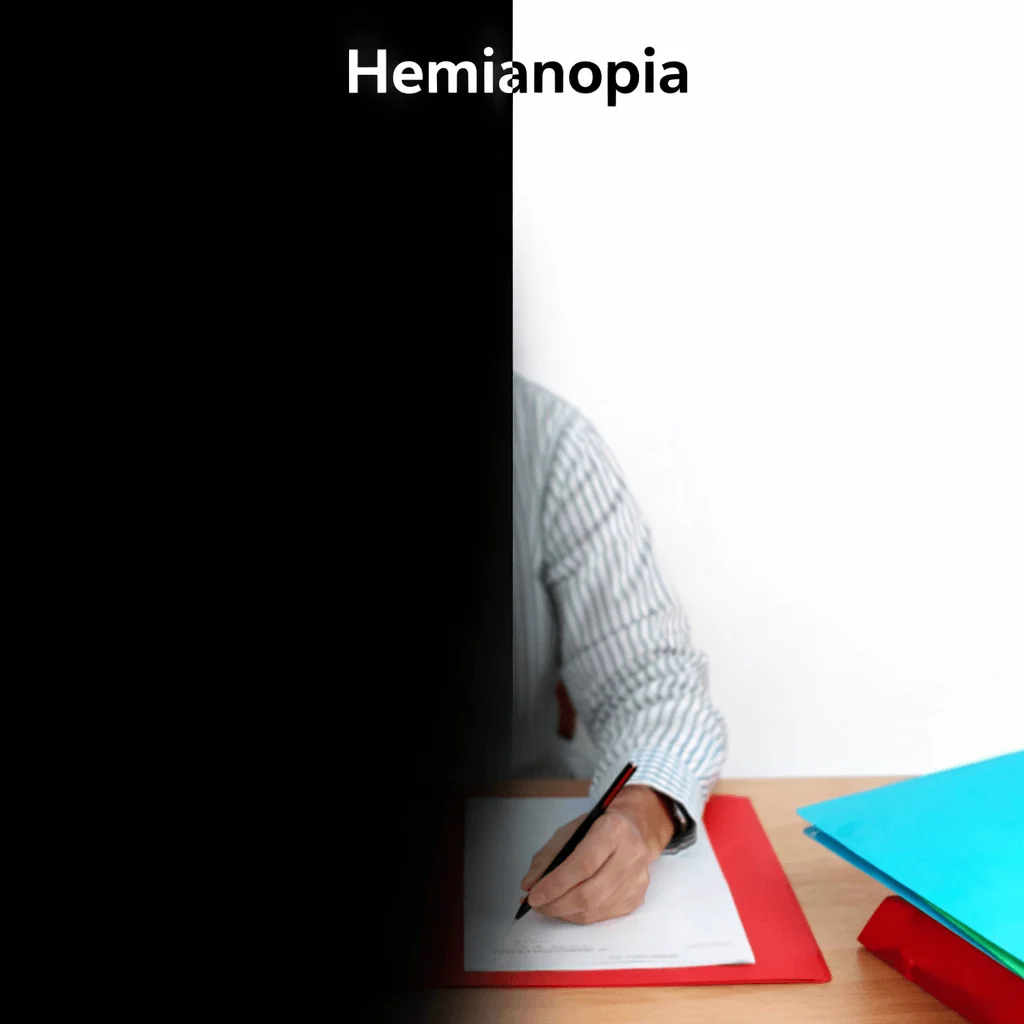
The result is bitemporal hemianopia: the right eye loses its right-side field and the left eye loses its left-side field, both respecting the vertical midline. Patients may bump into things on both sides or notice objects vanishing at the edges. Because the cause is frequently a mass, a bitemporal pattern typically prompts an MRI of the brain and the sellar region. When it appears suddenly with a severe headache, pituitary apoplexy - bleeding into a pituitary tumor - must be considered urgently.
Behind the Chiasm: Homonymous Patterns
Past the chiasm, the pathway carries one entire side of the visual world: the right optic tract and radiations handle the left half of vision for both eyes, and vice versa. So a lesion here produces a homonymous defect - the same side missing in both eyes.
A key refinement is congruity - how closely the two eyes' defects match. The farther back the lesion, the more identical the two eyes' fields become:
- Optic tract (just behind the chiasm) - an incongruous homonymous hemianopia, where the two eyes' defects differ somewhat in shape.
- Optic radiations - here the fibers split. The lower fibers swing forward through the temporal lobe (Meyer's loop) and carry the upper field, so a temporal lesion produces a superior quadrantanopia - a "pie in the sky." The upper fibers run through the parietal lobe and carry the lower field, so a parietal lesion produces an inferior quadrantanopia.
- Occipital cortex (the very back) - a highly congruous homonymous hemianopia, often with macular sparing: the central few degrees survive, because the macular representation is large and benefits from a dual blood supply. A stroke in the territory of the posterior cerebral artery is the textbook cause.
So a homonymous hemianopia that is nearly identical in both eyes and spares the center points to the occipital lobe, while one that is lopsided between the eyes points farther forward toward the tract - the same defect "shape," localized by its details.
A sudden, new loss of one side of vision in both eyes (a homonymous defect) can be a sign of a stroke at the back of the brain. Use BE-FAST - sudden trouble with Balance, Eyes (vision loss or double vision), Face drooping, Arm weakness, Speech difficulty - and if any are present, call 911 immediately. Posterior strokes can cause vision loss with few other symptoms, so do not wait for weakness or slurred speech to appear.
How the Pattern Localizes the Lesion
| Field pattern | Where it points |
|---|---|
| Central scotoma | Optic nerve or macula |
| Altitudinal (respects horizontal midline) | Optic nerve or retina |
| Arcuate | Optic nerve (classically glaucoma) |
| Bitemporal hemianopia | Optic chiasm |
| Incongruous homonymous hemianopia | Optic tract |
| Superior quadrantanopia ("pie in the sky") | Temporal lobe (Meyer's loop) |
| Inferior quadrantanopia | Parietal lobe |
| Congruous homonymous hemianopia with macular sparing | Occipital cortex |
The pattern is a starting point, not the final word. A central scotoma still needs imaging of the nerve and a look at the retina; a bitemporal pattern triggers an MRI; a homonymous pattern is worked up as a brain or stroke problem. Reliability matters too: fatigue, droopy lids, a lens rim, or poor fixation can manufacture a fake defect, which is why a subtle change is usually confirmed on a repeat visual field test before it is acted on. In children, a slowly progressive chiasmal or pathway defect can also reflect an optic pathway glioma, and in older adults a new altitudinal defect raises the question of giant cell arteritis.
What It Means for Driving
Driving standards account for peripheral field as well as central acuity. A homonymous hemianopia or a substantial bitemporal loss can fall below the standard for a license even when central acuity is sharp, because so much of the periphery needed to detect hazards and cross traffic is gone. The exact thresholds and rules vary by state and jurisdiction, so they should be checked locally, but the general principle holds: significant field loss can affect driving eligibility and safety, and it should be discussed honestly with your eye doctor. Our guide on driving with vision changes covers this in more depth.
Frequently Asked Questions
Can a field defect get better?
Sometimes. It depends entirely on the cause. Loss from optic neuritis may recover substantially; some homonymous defects after a stroke improve partially in the first months; glaucoma damage is permanent but treatment can stop it from worsening. The pattern, cause, and trend over time determine the outlook.
Why didn't I notice such a large blind area myself?
The brain is remarkably good at filling in and the other eye often covers part of the gap, so even a half-field loss can go unnoticed until it causes bumping into doorframes, missing words while reading, or near-misses while driving. This is exactly why formal field testing exists - it finds losses the basic eye chart misses.
My defect stops right down the middle. What does that tell the doctor?
A defect that ends cleanly at the vertical midline is a strong clue that the problem is at or behind the chiasm, where the pathway is organized by left versus right. A defect that respects the horizontal midline instead points toward the optic nerve or retina. That single observation steers the rest of the evaluation, including which scan is ordered.
Is a quadrantanopia less serious than a hemianopia?
Not necessarily - it is more about location than severity. A quadrant defect localizes to the temporal or parietal radiations, while a hemianopia suggests a larger or more posterior lesion. Both warrant a careful workup to find and address the underlying cause.
References
- American Academy of Ophthalmology. Standard Automated Perimetry. EyeWiki.
Medical Disclaimer: This information is for educational purposes only and does not replace professional medical advice.